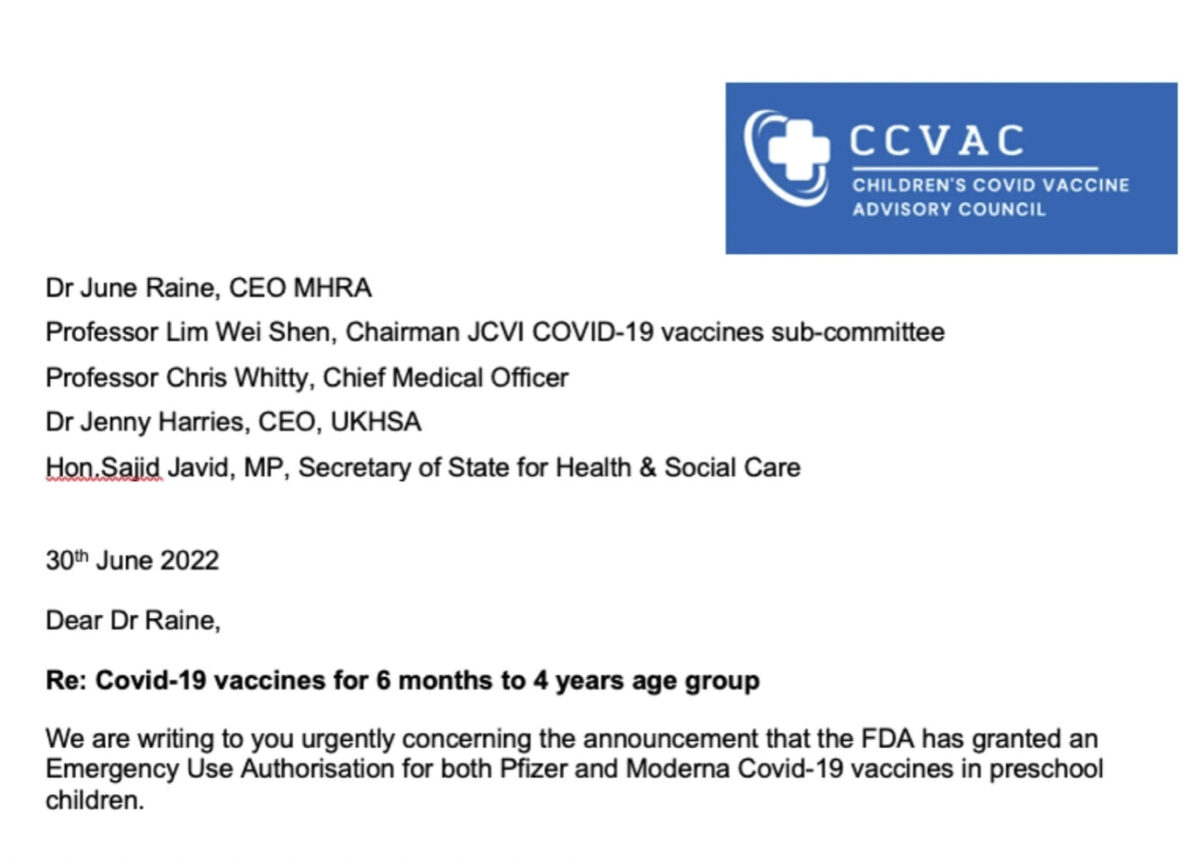
Below is a letter signed by 76 doctors in the UK, to the Medical and Healthcare products Regulatory Agency (MHRA) and other UK Government officials. This letter lays out comprehensive reasons why the recent U.S. FDA decision authorizing COVID vaccinations in infants and young children must not happen in the UK. The letter is well-sourced and accurate. Let us hope that main-stream media here in the United States and in the UK report on this letter in an unbiased fashion.