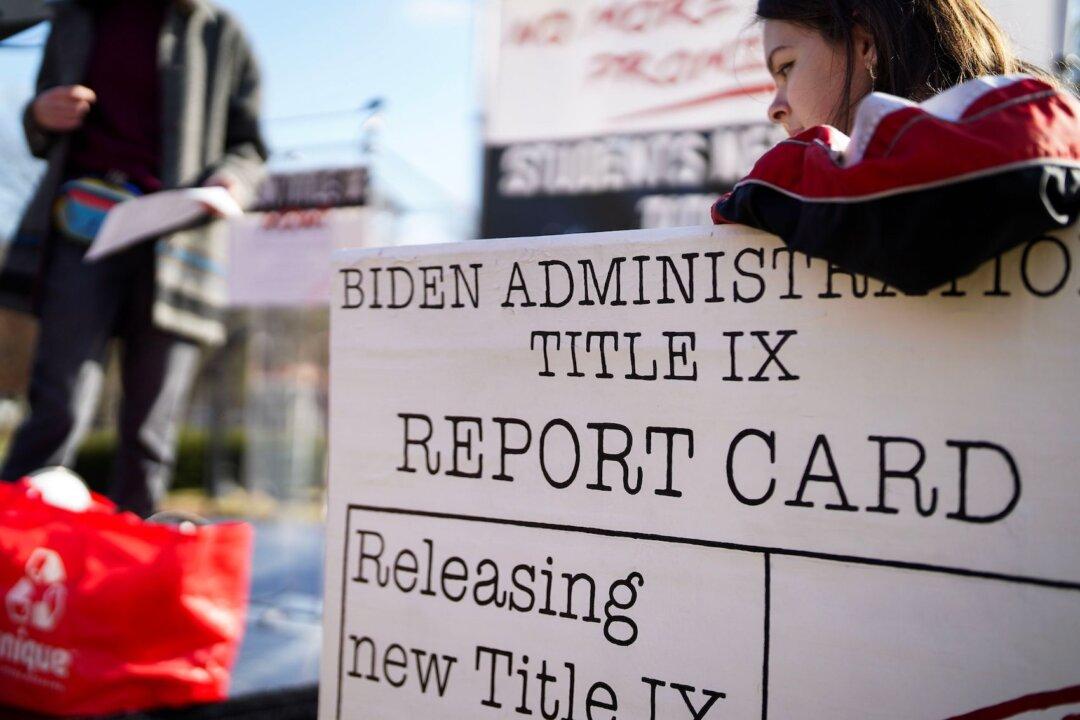
People rally against Bill C-14, the medically assisted dying bill, during a protest in Ottawa on June 1, 2016. Bill C-7, currently before the Senate, seeks to broaden the 2016 law on medical assistance in dying. The Canadian Press/Justin Tang
Federico Carboni made international news recently when he died in Italy’s first legal assisted suicide. Carboni wasn’t terminally ill. He was paralyzed from an auto accident. He sought suicide because he had no autonomy, saying in an interview, “I am like a boat adrift in the ocean.”
Wesley J. Smith
Author
Award-winning author Wesley J. Smith is host of the Humanize Podcast (Humanize.today), chairman of the Discovery Institute’s Center on Human Exceptionalism and a consultant to the Patients Rights Council. His latest book is “Culture of Death: The Age of ‘Do Harm’ Medicine.”