Adam Zivo: Canada’s Failed ‘Safer Supply’ Drug Experiment a Cautionary Tale for the World
Methamphetamine, heroin, and cocaine from a safe supply are handed out to drug users to mark International Overdose Awareness Day, in the Downtown Eastside of Vancouver on Aug. 31, 2021. Darryl Dyck/The Canadian Press
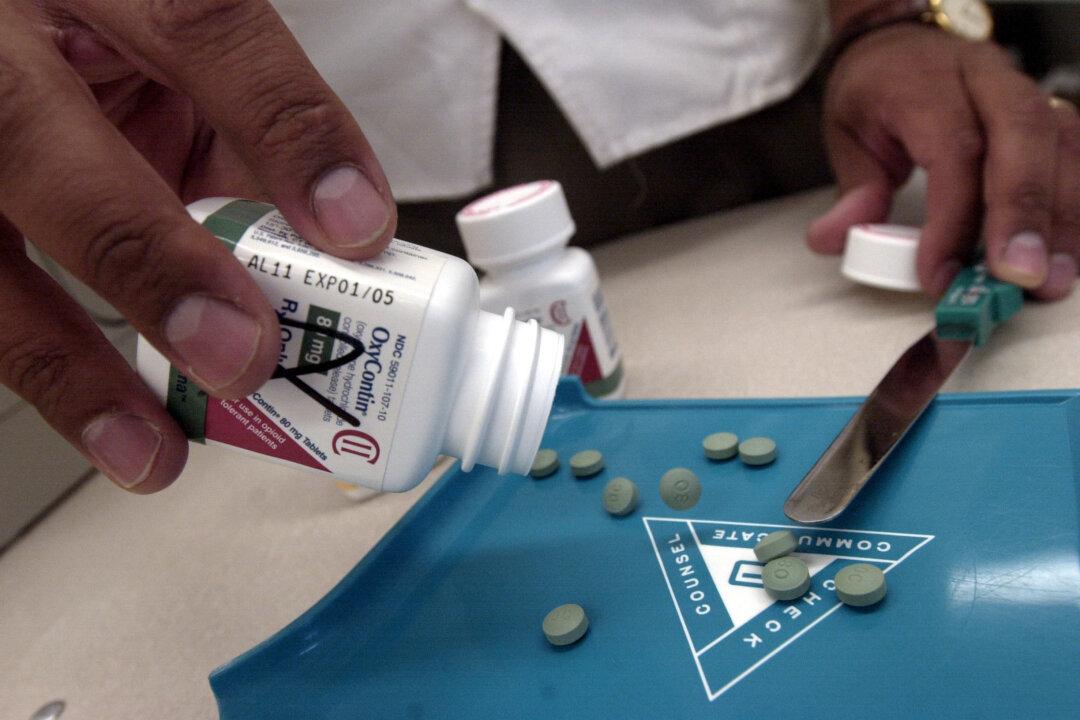
Faced with an overdose crisis that is killing thousands of people every year, Canada decided to embrace “safer supply,” a strategy that distributes free addictive drugs as an alternative to potentially tainted illicit substances. Yet the results have been disastrous and should serve as a cautionary tale for other jurisdictions.
Adam Zivo
Author
Adam Zivo is a political columnist based in Canada.