Dr. Armand Balboni, CEO of Appili Therapeutics Inc., said there’s a need for options to combat the virus at various stages, particularly “at the moment of exposure or confirmed infection.”
Antiviral drugs that target the CCP virus, particularly ones that are safe and can be “easily manufactured and distributed globally,” can fill the role in treating COVID-19 outside of a hospital setting.
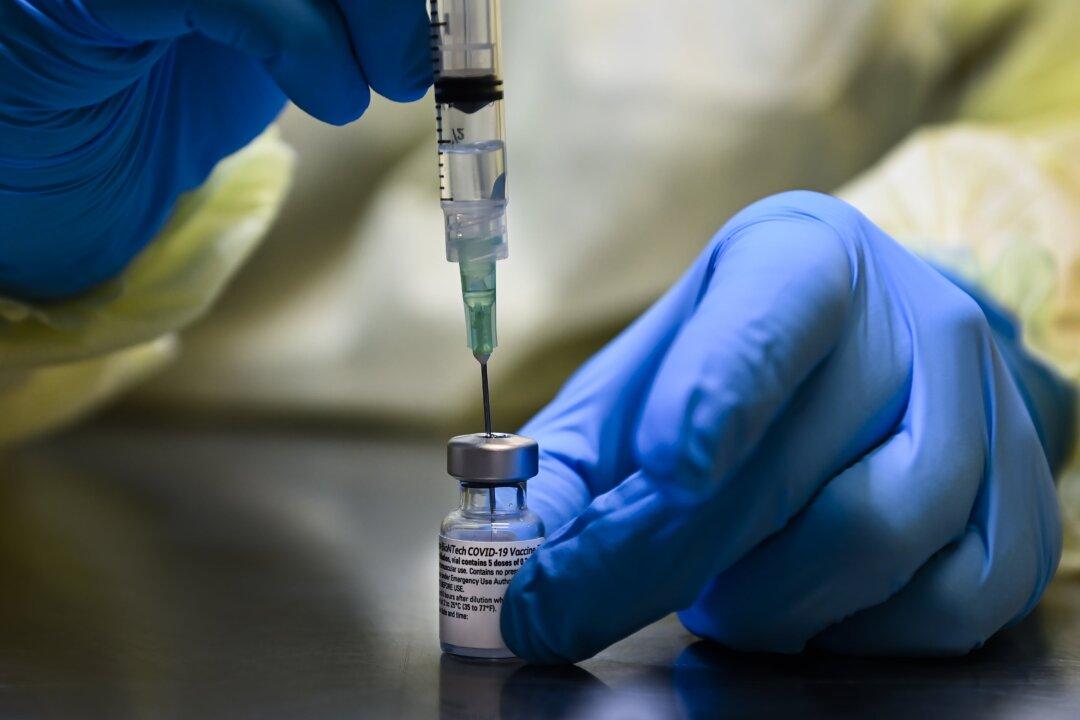
“These drugs are not intended to replace COVID-19 vaccines and other therapeutics for severely ill patients, but to cover aspects of disease management beyond the scope of vaccines and therapeutics for severe cases,” Balboni said.
Data shows that certain repurposed drugs can treat the early phase of COVID-19, so the scientific community and federal health agencies should be encouraging, instead of “discouraging, and in some cases prohibiting, the research and use of drugs that have been safely used for decades,” Johnson said.
“In fact, there has been a concerted effort to block doctors who actually treat COVID patients from compassionately using their ‘off label’ prescription rights for early treatment protocols.”
Scientists are finding that ivermectin—an oral drug that treats scabies, parasitic infections, river blindness, and rosacea in humans—is also effective in treating COVID-19. The drug is on the World Health Organization’s List of Essential Medicines.
Rajter says that ivermectin was soon adopted as part of the hospital’s treatment protocol for COVID-19, and more than seven months later, “the success rate of the Ivermectin based protocol is now far superior to what it was in its early days.”
He says more randomized controlled trials are needed to confirm the “preliminary findings” and address any safety concerns on the use of ivermectin. Yet, while his team “has multiple study protocols in place, ready to be implemented in short order,” funding and support for such a study has been difficult.
Dr. Pierre Kory, a pulmonologist at Aurora St. Luke’s Medical Center, said at the hearing that he and members of his organization at Frontline COVID-19 Critical Care Alliance have spent “almost nine months tirelessly reviewing the scientific literature to gain insight into this virus and the disease process and to develop effective treatment protocols” while treating COVID-19 patients.
“In the last three to four months, emerging publications provide conclusive data on the profound efficacy of the anti-parasite, anti-viral drug, anti-inflammatory agent called ivermectin in all stages of the disease,” Kory said.
“Ivermectin is highly safe, widely available, and low cost,” he said. “We now have data from over 20 well-designed clinical studies, 10 of them randomized, controlled trials, with every study consistently reporting large magnitude and statistically significant benefits in decreasing transmission rates, shortening recovery times, decreasing hospitalizations, or large reductions in deaths.”
“All I ask is for the NIH to review our data that we’ve compiled of all of the emerging data. ... We have immense amounts of data to show that it must be implemented and implemented now.”
The FDA says ivermectin “should be avoided,” as its benefits and safety haven’t been established and that “testing is needed to determine whether ivermectin might be appropriate” for prevention and treatment of COVID-19.
Information about ivermectin hasn’t been updated since Aug. 27 on the NIH’s website, or since May 1 on the FDA’s website, although more clinical data have been published about the drug in preventing and treating COVID-19.

Other COVID-19 treatments such as monoclonal antibodies and dexamethasone have been granted emergency use authorization by the FDA.
Dr. Jay Bhattacharya says the lack of funding for randomized trials on existing drugs for early intervention of COVID-19 is leaving some scientists and physicians to not prescribe certain drugs or other therapies despite their effectiveness.
Bhattacharya, a professor of medicine at Stanford University, says this is where the NIH can play a role.
“In principle, the NIH exists to solve this market failure,” Bhattacharya says. “It could and should use its resources to help fund randomized evaluations of these drugs for off-label purposes.”
Attacked by Media
Johnson said that prior to the hearing, he and the physicians were attacked by media calling it “dangerous, and instead of waiting until after the hearing to trash this information and our witnesses, The New York Times and other publications have already run pre-emptive attacks, implying this hearing is anti-vaccine.”Balboni, a life-long Democrat and a subscriber to the NY Times, says he almost didn’t participate in the hearing. “I have to say, I was quite dismayed this morning and almost didn’t participate when I saw the news that I was participating as a fringe member of an anti-vaccine group,” Balboni said. “That couldn’t be further from the truth.”
Sen. Gary Peters (D-Mich.), the only Democrat present at the hearing, in his opening statement before walking out, accused the committee of being “used as a platform to attack science and promote discredited treatments.”
“Sadly, it appears that today’s hearing will follow the same path, playing politics with public health, and will not give us the information we need to tackle this crisis,” Peters said. “The panelists have been selected for their political, not their medical, views.”
The other Democrat members refused to attend the hearing. Five Republicans also didn’t attend.
Johnson said he doesn’t understand the “concerted effort to silence the voices” of health professionals promoting early treatments for COVID-19.